
Quick answer
In the first 4-6 weeks of a NSW psychological injury claim, there is no perfect sequence. WHS, HR, liability, treatment and return-to-work planning usually run in parallel and loop back. The realistic aim is to keep early support and information-gathering moving while liability is being worked through, communicate consistently, and recognise where psychosocial issues need WHS attention alongside the claim.
Key Takeaways
- The first 4-6 weeks of a psychological injury claim set the trajectory, and decisions are usually made with incomplete information.
- SIRA Standard 33 and psychosocial WHS duties have raised expectations for early, practical and empathetic claim handling.
- Section 11A reasonable management action is evidence-heavy and often fails where causation is mixed.
- Treatment and basic RTW planning can usually proceed without prejudice while liability is being worked through.
- Rehab referrals only help when insurers and employers are ready to act on recommendations.
Psychological injury claims in NSW are no longer edge cases. They are more frequent, more expensive and harder to turn around than many physical injuries. How the first month is handled can either steady the claim or lock in long-running problems.
This article is written from a NSW workers' compensation and WHS perspective. It is aimed at:
insurer claim staff and technical specialists employer RTW coordinators, HR and WHS leads workplace rehabilitation providers
It focuses on the first 4–6 weeks after a psychological injury claim is notified, when decisions about contact, support, liability and work need to be made with incomplete information.
The aim is not to offer a perfect sequence. Many real files loop back, stall, or move in jumps. The goal here is to name the main tensions and give a realistic sense of what "roughly right" can look like in that early window.
This article uses plain language and avoids stock buzzwords, so it stays readable for busy scheme users.
Why psychological injury handling is under more pressure
Claim trends
NSW and national data show psychological injury claims growing faster than physical ones and consuming a bigger slice of scheme cost.
National figures tell a similar story on duration and recovery:
Safe Work Australia data and NSW Treasury commentary link this pattern to growing pressure on scheme sustainability and on employers' labour costs. This means more scrutiny on how psychological injury claims are managed, especially early on.
- Accepted psychological injury (mental health) claims in NSW rose by around 30% over the four years to mid-2023, compared with about 11% growth in physical injury claims.
- Psychological injury claims comprise roughly 12% of NSW workers' compensation claims but around 38% of scheme costs. The average cost per psychological injury claim in NSW has roughly doubled from about $146,000 in 2019–20 to about $288,500 in 2024–25.
- Median time lost for mental health claims is about 34 weeks, compared with roughly 8 weeks for other injuries.
- Around 40% of workers with psychological injuries are still off work 12 months after injury, while most physical injury claimants are back at work within the first quarter.

Regulatory settings and expectations
Over roughly the same period, NSW WHS and compensation rules have moved decisively toward psychosocial risk.
SafeWork NSW's Psychological Health and Safety Strategy 2024–2026 commits to a marked lift in compliance activity, including a target of 25% more inspector visits each year and psychosocial WHS checks on visits to large workplaces.
On the workers' compensation side:
This regulatory mix means that when a psychological claim lands, insurer and employer behaviour in the first month is no longer just a "service" issue. It can go to compliance.
- In October 2022, NSW amended its Work Health and Safety Regulation so that psychosocial risks must be identified, assessed and controlled in the same structured way as physical hazards, supported by an approved Code of Practice.
- The Code and related material list hazards such as high job demands, low job control, poor support, bullying and harassment, exposure to violence or traumatic events, low role clarity and poorly managed organisational change.
- SIRA's Standard of Practice 33 (March 2021) expects insurers to handle psychological injury claims with early, empathetic contact, prompt access to treatment and active recovery and return-to-work planning, and it reserves the right to audit and sanction insurers who fall short.
- Employers must not terminate a worker within six months of a work-related injury solely because of that injury and must provide suitable duties where reasonably practicable, including for psychological injuries.
Getting clear on terms: injury, stress and psychosocial risk
What counts as a psychological injury in the scheme
Under NSW workers' compensation law, a psychological injury is generally a diagnosable psychological or psychiatric disorder that arises out of or in the course of employment. Common diagnoses include depression, anxiety disorders, post-traumatic stress disorder and adjustment disorder.
Work must be at least a substantial contributing factor (or, for some disease concepts, the main contributing factor) to the condition. A worker feeling "stressed" or unhappy, without a diagnosis linking symptoms to work factors, does not in itself meet the threshold.
Evidence is both subjective and objective:
The Personal Injury Commission (PIC) weighs the full chronology of work events, the medical opinions and any alternate explanations. It has also been clear that the worker's genuine perception of real events matters in causation, even when the employer remembers those events differently.
- the worker's account and perceptions
- medical reports from GP, psychologist or psychiatrist
- workplace material such as emails, witness statements and HR files.
Stress versus a compensable injury
Many files start with language like "stress leave", "burnout" or "anxiety at work". In the early weeks, there is often a moving target: a GP may write "stress" on the first certificate, then later adopt a more precise diagnosis once assessment is complete.
Case managers and employers often feel a dilemma:
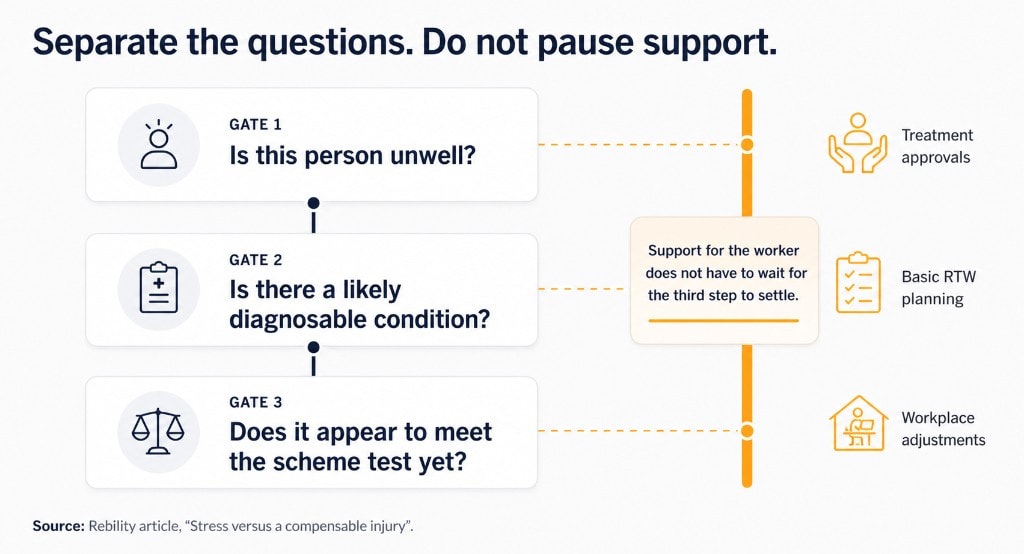
A workable early approach is to separate three ideas:
Support for the worker does not have to wait for the third step to settle. Treatment approvals, basic RTW planning and workplace adjustments can start while the technical liability decision is still forming.
- If the claim is treated as "just stress", the worker may feel dismissed and disengage.
- If every tense situation is framed immediately as a psychological injury, workers can be nudged into a sick-role that may not fit, and scheme costs rise without better outcomes.
- Is this person unwell?
- Is there a likely diagnosable condition?
- Does it appear to meet the scheme test yet?
Psychosocial hazards and WHS duties
Separate from the question of a compensable injury is the WHS duty to manage psychosocial hazards.
The NSW Code of Practice and national material describe psychosocial hazards such as: high job demands, low job control, poor support or recognition, bullying and harassment, exposure to violence or traumatic events, lack of role clarity and badly managed change.
Employers must identify where these hazards exist, assess the risk they pose and implement controls. That duty applies regardless of whether a claim is lodged or accepted.
A psychological injury claim often exposes an underlying psychosocial issue that has been building for months or years. Early claim handling then needs to run in parallel with WHS steps such as:
This is one place where friction appears. Some employers fear that acknowledging a psychosocial hazard looks like an admission of legal fault. WHS law pulls in the opposite direction: hazards must be controlled whether or not the claim ends up accepted.
- reviewing workloads, rosters, staffing or supervision
- checking whether bullying or conflict reports have been addressed
- looking at whether team-level changes are needed, not just individual support.
Where early friction comes from
Liability decisions versus early support
Standard 33 and the Guidelines push insurers to act quickly and with empathy. At the same time, the scheme expects sound liability decisions based on evidence. Those expectations can clash, especially when:
On one hand, paying for early treatment and talking about return to work can feel risky to some insurers if they think a defence might later apply. On the other, delaying all support until every document is in can leave a distressed worker with no clear pathway, and that delay itself can worsen outcomes.
A common middle path in the first month is to:
That path still has downsides. Some workers will read any delay or neutral wording as disbelief. Some employers will worry the insurer is "giving in". There is no version that keeps everyone comfortable. Recognising that tension helps manage expectations.
- the account of events is strongly contested
- there is an active grievance, misconduct or performance process
- documentation is patchy or slow to emerge.
- fund reasonable early treatment on a "without prejudice" basis while facts are gathered
- explain to the worker that the liability decision is still open, but that their health and income are being stabilised in the meantime
- keep written communication measured and factual, avoiding language that sounds like a final verdict before evidence is complete.
Reasonable management action and contested stories
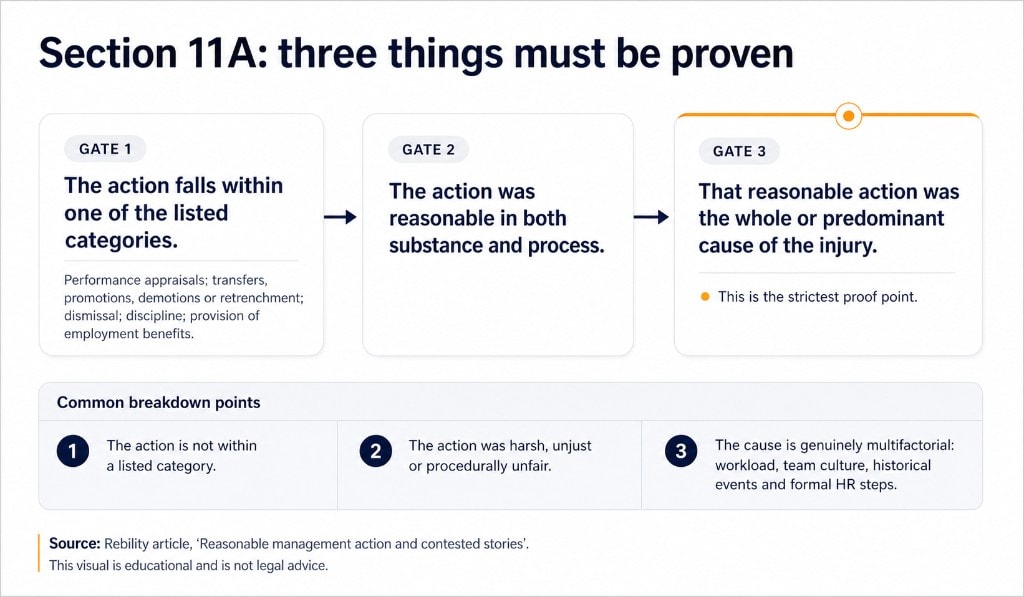
Section 11A of the Workers Compensation Act creates an important carve-out. An employer is not liable for a psychological injury that is wholly or predominantly caused by reasonable action taken (or proposed) by the employer in relation to specific areas such as:
To rely on this defence, the employer (and insurer) must prove three things:
The onus is firmly on the employer, on the balance of probabilities. If the action was harsh, unjust or procedurally unfair, it will not qualify as "reasonable action". And even when action is reasonable, many psychological injuries have mixed causes – workload, team culture, historical events and formal HR steps. Where the cause is genuinely multifactorial, the s11A defence will often fail.
PIC case law also stresses that the worker's perception of real events has to be weighed, not just the employer's description.
- performance appraisals
- transfers, promotions, demotions or retrenchment
- dismissal
- discipline
- provision of employment benefits.
- The action falls within one of those listed categories.
- The action was reasonable in both substance and process.
- That reasonable action was the whole or predominant cause of the injury.
Trust and communication gaps
Psychological injury files often start with strained relationships:
The early calls here are delicate. Standard 33 pushes for contact with the worker within a short timeframe, in a way that feels human and not interrogatory.
Some traps that experienced practitioners watch for in this first contact phase:
Managing those gaps often involves extra coordination work: additional calls, checking wording with HR before letters go out, and correcting misunderstandings as they arise.
- The worker may feel they have already tried internal complaint paths and not been heard.
- The employer may feel blindsided by a claim lodged "out of the blue", or resentful if it follows a difficult performance process.
- The insurer receives a referral that might be little more than a certificate and a short claim form.
- Investigative tone too early.
- Mismatch of messages between calls and letters.
- Mixed signals between insurer and employer about work status.
Working the first 30 days
There is no single correct sequence for the first month. WHS and HR processes, liability decision-making, treatment and RTW planning often run alongside each other and loop back.

First contact and tone
Standard 33 expects early, person-to-person contact from the insurer – often within a few business days of the claim. The first call is less about solving everything and more about establishing a respectful, trustworthy link.
Elements that tend to help:
Real-world complications include:
In those cases, other channels (SMS, email, letters, involving a rehab provider or GP case conference) may be needed.
- Plain introductions: who you are, why you are calling, and what your role is.
- Short calls when needed for workers in acute distress.
- Clear explanation of next steps while evidence is being gathered.
- Workers who will not take calls from unknown numbers.
- Employers who ask the worker not to speak before HR/legal advice.
- Language or cultural barriers.
Building a picture of work and psychosocial conditions
To make reasonable early decisions, insurers and rehab providers need a workable picture of:
The aim is not a full workplace investigation. Three lines of enquiry are often enough for a first pass:
Talking with both worker and employer matters. The question in the early weeks is not "who is right?", but "does this sound like a plausible work-related pathway to the reported condition, and what information is still missing?".
- what the job actually looks like
- what changed in the lead-up to the injury
- what known psychosocial hazards are present.
- Role and pattern of work.
- Recent changes.
- Existing WHS or HR signals.
Recovery and work: keeping options open
The evidence base in Australia increasingly supports staying connected with good work, where that is safe, as part of recovery from mental health conditions.
In the first month, case managers are usually juggling:
A few practical anchors:
There are cases where pushing for early RTW is simply unsafe. In those files, the early weeks may be about stabilising health and securing income while WHS and organisational issues are worked on.
- certificates that may state "unfit for any work"
- a worker who says they cannot face the workplace
- an employer who either wants the worker back immediately, or does not want them back at all.
- Separate "this workplace" from "any work".
- Give doctors a concrete picture of duties.
- Expect the path to zigzag.
Using support services without handing the file away
Psychological injury files often involve several helpers: rehab providers, EAP, internal HR and WHS specialists, and sometimes external mediators.
Workplace rehab providers in particular are expected to bring mental health knowledge, coordination skills and a realistic RTW focus.
A few common snags:
In short, support services work best when the insurer and employer stay actively engaged rather than treating the referral as a way to park a hard file.
- "Referral as offload" when recommendations are not actioned.
- Confused roles between worker advocacy and coordination role.
- Over-reliance on counselling without structural workplace controls.
Two familiar claim patterns in the early weeks
Every file has its own twists, but two patterns show up often enough to be worth naming.
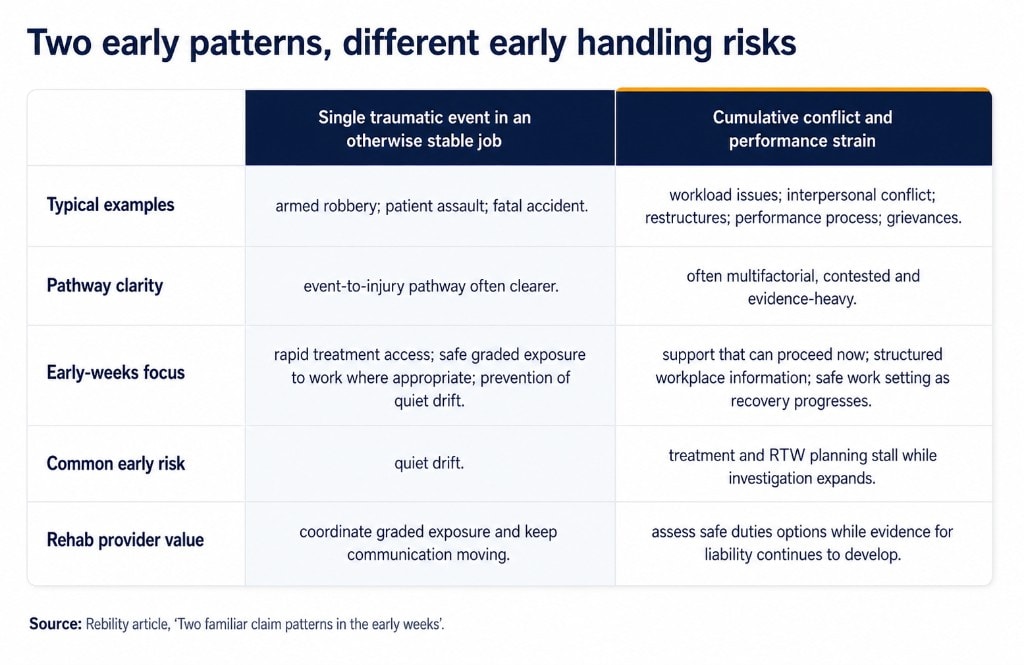
Single traumatic event in an otherwise stable job
Examples include:
Here, the pathway from event to injury is often clearer. Early-weeks focus usually includes rapid treatment access, safe graded exposure to work where appropriate, and prevention of quiet drift.
- a retail worker experiencing an armed robbery
- a nurse assaulted by a patient
- a driver involved in a fatal accident.
Cumulative conflict and performance strain
The second pattern is the slow-burn file: long-standing workload issues, interpersonal conflict, restructures, clashing expectations about performance, grievances, and then a claim.
Here, there is often:
These files can become investigation-heavy while treatment and RTW planning stall. Practical early questions are what support can proceed now, and whether there is any safe work setting that can be made viable as recovery progresses.
- an active or recent performance process or misconduct allegation
- s11A being raised early as a potential defence
- multiple witnesses with different memories of events.
Practical example
A cumulative conflict claim enters week three with active HR process steps, contested facts, and a worker certifying unfit. The insurer funds early treatment without prejudice, sets neutral communication expectations, obtains structured workplace information, and coordinates a rehab provider to assess safe duties options while evidence for liability continues to develop.
When to consider a referral
Consider referral when duties are unclear, relationships are strained, or workplace changes are needed to reduce psychosocial risk while supporting recovery.
Interested in Psychological Support?
Recovery-focused support for workers with psychological barriers affecting work participation.
Learn MoreFrequently asked questions
Usually no. Early treatment access, income communication and practical RTW planning can proceed while liability is still being worked through, provided communication is clear about what is provisional.
Both extremes tend to fail in practice. Non-urgent escalatory steps may need to pause, while safety-critical processes continue with added support and procedural fairness.
Keep contact channels open without pressure, use clear written updates, and coordinate through treating providers where direct contact is limited.
Early engagement usually helps when duties are unclear, conflict is affecting planning, or treating doctors need practical workplace detail to certify capacity.
Provide concrete suitable-duties detail, offer case conferencing, and stay open to alternative placements where the original setting cannot be made safe.
Treat section 11A as an evidence question, not a foregone conclusion. Gather category, reasonableness and predominant-cause evidence methodically while continuing practical support.
References
- Psychosocial Risk and Psychological Injury in NSW: A Comprehensive Research Brief — Rebility
- Workers Compensation Guidelines and Standard of Practice 33 — State Insurance Regulatory Authority (SIRA) Source
- Code of Practice: Managing Psychosocial Hazards at Work — SafeWork NSW Source
- Psychological Health and Safety Strategy 2024-2026 — SafeWork NSW Source
- Psychological health and safety in the workplace - Snapshot — Safe Work Australia Source
- Selected decisions including Toll Pty Ltd v Lee and Colin Joss & Co Pty Ltd v Williams — Personal Injury Commission (NSW)
- NSW Treasury and government publications on workplace mental ill-health costs — NSW Government


